| dc.description.abstract | INTRODUCTION: Penetrating atherosclerotic ulcers (PAU) develop in the internal elastic lamina and indicate severe aortic atherosclerosis. PAU can have an associated intraluminal aortic thrombus, with associated risk of thromboembolism with subsequent mesenteric infarct and limb loss. We present a case of persistent descending thoracic aortic thrombus, with embolic renal infarcts, necessitating repair.
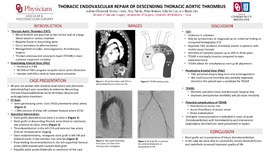
CASE DESCRIPTION: A 80-year-old woman with history of bilateral renal infarcts on Eliquis and uncontrolled hypertension was referred to our department for extensive aortic atherosclerosis and 6mm ulceration proximal to the celiac artery, demonstrated on a CT. A follow up Computed Tomography Angiogram (CTA) demonstrated a persistent descending thoracic aortic thrombus and thoracic endovascular repair (TEVAR) was indicated. Preoperative imaging demonstrated >50% stenosis of the distal left common femoral artery (CFA).
We accessed the proximal left CFA and subsequently placed stent grafts in the descending thoracic aorta, distally to proximally. Completion aortogram revealed complete occlusion in left external iliac artery. Doppler signals to the left foot were diminished on prompt exam.
Current intraoperative imaging showed thromboembolism vs. flow-limiting dissection in the left CFA and external iliac arteries. Given these findings, an open endarterectomy of the iliac arteries was indicated, along with stent graft deployment in the left external iliac artery and bilateral stents in the common iliac arteries.
A complete angiogram revealed a flow-limiting thromboembolism in the left superficial femoral artery (SFA). This was treated with covered stent placement, excluding the thrombus. Subsequent imaging demonstrated brisk flow into the left foot. On exam, pulses were palpable in the feet bilaterally and she moved all extremities. This patient had an uneventful hospital course and was discharge on postoperative day three.
DISCUSSION: PAUs are a collective part of Acute Aortic Syndrome (AAS), seen in 2-8% of patients with AAS. PAUs develop from aortic mural thrombi, located most frequently in the abdominal aorta. A PAU > 4mm thick with ulceration is categorized as a complex plaque and warrants surgical repair. Anticoagulation is not sufficient for complex plaques. Endovascular repair (EVAR) is preferred to open since operating time is shorter, involves smaller incisions, and decreased hospital stay, with improved perioperative morbidity and all-cause mortality. Employing quality vascular access and wire manipulation can reduce endoleaks, access complications, and peripheral embolization. If complications arise, prompt imaging to access the stenotic vessels is necessary. This case demonstrates the potential morbidity of aortic thrombus embolization and the attention to detail required for successful treatment. | en_US |