| dc.contributor.author | Haney, Taryn | |
| dc.contributor.author | Harris, Kelley | |
| dc.contributor.author | Livingston, Reagan | |
| dc.contributor.author | Nadimpalli, Suma | |
| dc.date.accessioned | 2023-11-02T20:47:16Z | |
| dc.date.available | 2023-11-02T20:47:16Z | |
| dc.date.issued | 2023-02-17 | |
| dc.identifier | ouhd_Haney_rarecasereportofanadultwith_2023 | |
| dc.identifier.citation | Haney, T., Harris, K., Livingston, R., and Nadimpalli, S. (2023, February 17). A rare case report of an adult with rapidly progressive glomerulonephritis secondary to severe IgA vasculitis. Poster presented at Research Week, Oklahoma State University Center for Health Sciences, Tulsa, Ok. | |
| dc.identifier.uri | https://hdl.handle.net/11244/339938 | |
| dc.description.abstract | Background: IgA nephropathy is a common form of glomerulonephritis (GN) with an estimated incidence of two per 100,000 adults. A small portion of these cases will advance to rapidly progressive glomerulonephritis (RPGN). Risk factors include older age, purpura, elevated antistreptolysin O titer, and low complement C3 levels. | |
| dc.description.abstract | A common clinical sign is gross hematuria. Significant proteinuria is also noted prompting a GN evaluation. Another common manifestation is palpable purpura. Although, this classic rash is not present in approximately 25% of cases at time of diagnosis. | |
| dc.description.abstract | Diagnosis is heavily based on clinical presentation thus underscoring the need for clinical suspicion. Lab tests support diagnosis, however, the definitive method is via biopsy. Pathology will reveal leukocytoclastic vasculitis with IgA deposition. | |
| dc.description.abstract | Mainstay of therapy focuses on limiting progression by reducing proteinuria to a goal of less than one gram per day. Renin-angiotensinogen-aldosterone inhibitors are initially utilized followed by the addition of glucocorticoids if excessive proteinuria persists. If RPGN develops the degree of immunosuppression is advanced. | |
| dc.description.abstract | This report explores a case of IgA vasculitis in an older adult brought on by a streptococcal infection with manifestations of RPGN and palpable purpura. | |
| dc.description.abstract | Case Presentation: A 72-year-old male presented reporting generalized weakness and fatigue that worsened over a few months. Labs revealed an elevated creatinine of 12.02 and significant proteinuria. Further workup included low complement levels, equivocal PR3 ANCA level, and negative glomerular basement membrane antibody, ANA, and cryoproteins. Four of four blood cultures did return positive for Streptococcus. Antistreptolysin O and DNase-B antibodies were later found to be negative. However, given this presentation there was a high suspicion for post-streptococcal GN. | |
| dc.description.abstract | Due to significant thrombocytopenia, a renal biopsy was postponed, and antibiotics continued for the bacteremia which were completed during hospitalization. | |
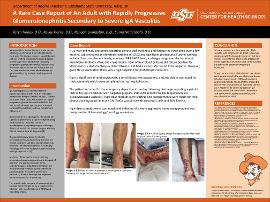
| dc.description.abstract | The patient returned to the emergency department the day following discharge reporting a painful rash to his legs consistent with palpable purpura. ESR >140 and CRP 67.86. Biopsy revealed leukocytoclastic vasculitis. | |
| dc.description.abstract | High-dose steroids were started, and arrangements were made for renal biopsy showing pauci-immune GN (ANCA vasculitis) with crescentic cells and 20% fibrosis. High-dose steroids were continued, and initiation of a more aggressive immunosuppressant was postponed until hematology/oncology evaluation. | |
| dc.description.abstract | Discussion: This case presents a unique example of IgA vasculitis with progression to RPGN following a streptococcal infection and the use of high-dose steroids in an effort to prevent the progression to end stage renal disease (ESRD). Unfortunately, this patient did become hemodialysis dependent. | |
| dc.description.abstract | Though, rare in adults, clinical trials have shown worse outcomes with the use of glucocorticoids including progression to ESRD and long-term gastrointestinal side effects. This probes the necessity for re-evaluation of high-dose steroids use in moderate-to-severe episodes of IgA vasculitis versus the use of other treatments such as rituximab, cyclophosphamide, and mycophenolate mofetil. | |
| dc.format | application/pdf | |
| dc.language | en_US | |
| dc.publisher | Oklahoma State University Center for Health Sciences | |
| dc.rights | The author(s) retain the copyright or have the right to deposit the item giving the Oklahoma State University Library a limited, non-exclusive right to share this material in its institutional repository. Contact Digital Resources and Discovery Services at lib-dls@okstate.edu or 405-744-9161 for the permission policy on the use, reproduction or distribution of this material. | |
| dc.title | Rare case report of an adult with rapidly progressive glomerulonephritis secondary to severe IgA vasculitis | |
| osu.filename | ouhd_Haney_rarecasereportofanadultwith_2023.pdf | |
| dc.type.genre | Presentation | |
| dc.type.material | Text | |
| dc.subject.keywords | vasculitis | |
| dc.subject.keywords | IgA nephropathy | |
| dc.subject.keywords | rapidly progressive glomerulonephritis | |