| dc.description.abstract | INTRODUCTION: The development of valvular incompetence and/or obstruction in the pelvic and gonadal veins causing disabling symptoms comprises Pelvic Congestion Syndrome (PCS). It is a less known pathologic condition commonly occurring in women of child bearing age, and diagnosis can be challenging due to a variety of clinical presentations. Nutcracker syndrome (NCS) is a potential cause of PCS and involves compression of the left renal vein between the superior mesenteric artery and the aorta. We report one such case of a woman who presented with chronic pelvic pain.
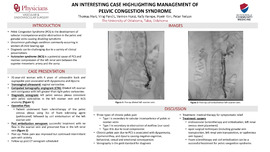
CASE DESCRIPTION: Our patient is a 31-year-old woman evaluated in our clinic with 6 years of unbearable back and suprapubic pain associated with dyspareunia and dysuria. She underwent evaluation by her gynecologist, and a transvaginal ultrasound demonstrated vaginal varicosities. Computed tomography angiogram (CTA) showed dilated left ovarian vein contiguous with left greater than right pelvic varicosities. We then performed a diagnostic venogram that demonstrated left pelvic venous plexus consistent with pelvic varicosities in the left ovarian vein and NCS anatomy. We decided to treat the PCS first. The patient underwent foam sclerotherapy of the pelvic venous plexus using 3cc of foam sclerosing agent (polidocanol) followed by coil embolization of the left ovarian vein. Post embolization venogram demonstrated radiographically successful treatment with no flow in the ovarian vein and preserved flow in the left renal vein.
DISCUSSION: Chronic pelvic pain due to pelvic congestion is often associated with a constellation of symptoms including pelvic pain, dyspareunia, dysmenorrhea, and dysuria causing negative cognitive, behavioral, sexual and emotional consequences. There are three types of chronic pelvic pain, categorized by etiology. Type I is secondary to valvular incompetence of pelvic or ovarian veins, Type II is secondary to obstruction of outflow, and Type III is due to local compression. Venography is the gold standard for diagnosis. Treatment is directed at providing symptomatic relief with medical therapy, and treating the underlying cause by either endovascular (sclerotherapy and embolization, left renal venous stent placement) or open surgical techniques (including gonadal vein transposition, left renal vein transposition, or saphenous vein bypass). | en_US |