| dc.description.abstract | INTRODUCTION: Atherosclerotic renal artery stenosis causes hypertension that is resistant to medical management and may eventually lead to loss of kidney function. The treatment options for uncontrolled hypertension include best medical therapy (BMT), renal artery stenting (RAS), or surgical intervention; however, the optimal modality remains uncertain. This is the case of a patient with renal artery stenosis complicated by concurrent obstructive uropathy.
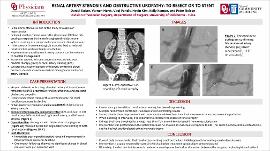
CASE DESCRIPTION: Our patient is a 66-year-old male with a long-standing history of hypertension uncontrolled with BMT (beta blocker, angiotensin II receptor blocker (ARB) and a thiazide diuretic) and progressive renal insufficiency which was presumed to be due to prostatic obstructive uropathy. Despite undergoing a transurethral prostatectomy, his renal function continued to decline. A pelvic magnetic resonance angiogram (MRA) was performed which showed bilateral renal artery stenosis with the left being worse than the right. Computed tomography angiogram (CTA) was then performed which confirmed significant bilateral renal artery stenosis of 80 percent and 60 percent of the left and right renal artery respectively. The patient then underwent balloon angioplasty followed by stenting of both vessels without complication. Post-stenting angiography showed less than 30 percent stenosis of either vessel. During hospitalization, he had some improvement in his blood pressure, and his renal function was improved from baseline. One month follow up showed no significant change in blood pressure from initial visit prior to stenting.
DISCUSSION: In healthy subjects, reduced renal perfusion lowers the glomerular filtration rate (GFR), causing a response by the renin-angiotensin-aldosterone system (RAAS) which leads to a compensatory increase in blood pressure. Although the GFR is reduced, renal parenchyma is able to adapt to reduced blood flow if perfusion pressure is reduced by 40 percent. There are a number of ways to manage renal artery stenosis, including RAS versus BMT. Currently, the effects of stenting are controversial and not fully understood. Multiple randomized trails have shown confounding results. Some trails have shown benefit in RAS, while others have demonstrated increase adverse outcomes due to renal reperfusion. In this case, we decided to to proceed with RAS given the significant stenosis on imaging, the patient's clinical presentation of worsening renal function despite BMT, and having ruled out other causes of progressive renal failure. The decision to intervene in these patients is usually determined on a case-by-case basis after discussion between surgeon, nephrologist and patient and after educating the patient on the risks and benefits. | en_US |