Enteric Duplication Cyst in a Patient with Suspected Milk-Protein Allergic Proctocolitis
Date
2020-05Metadata
Show full item recordAbstract
INTRODUCTION: Gastrointestinal duplication cysts are rare congenital malformations that are typically discovered by routine prenatal ultrasound. These cysts can arise anywhere along the gastrointestinal tract but are most commonly found in the small intestine. Presenting symptoms vary, but often include: nausea, vomiting, abdominal pain or distention, obstruction, or a palpable mass.
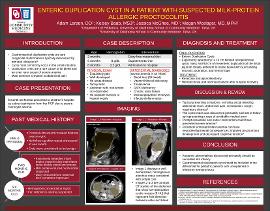
CASE DESCRIPTION: An exclusively breastfed eight-month-old female presented to the children’s hospital with severe microcytic anemia (hemoglobin concentration of 3.2 g/dL). Past medical history was significant for a six-month history of emesis and intermittent hematochezia. Around two months of age, she presented to the pediatrician due to intermittent loose, bloody stools, which were attributed to milk protein-induced proctocolitis. Dairy was removed from the mother’s diet, which reportedly provided some improvement. Iron deficiency anemia was diagnosed at four months of age when hemoglobin concentration was 8 g/dL and improved to 10.6 g/dL at six months after the initiation of iron therapy. Follow-up labs at eight months revealed severe microcytic anemia and prompted admission to the children’s hospital. Notably, medical history included a prenatal ultrasound concerning for bilateral ovarian cysts. Repeated postnatal images revealed decreased size of the cysts, and they were deemed insignificant. Upon admission, the patient was pale and tachycardic, but otherwise well appearing with a soft, non-tender, non-distended abdomen, normal bowel sounds, no palpable masses or hepatosplenomegaly. Ultrasound and CT of the abdomen showed bilateral abdominal mesenteric masses favoring mesenteric cysts. Exploratory laparotomy identified a ten cm bilobed retroperitoneal cystic mass and 80 cm of mesenteric duplication at the distal jejunum and proximal ileum closely adherent to native tissues with surrounding mucosal necrosis, ulceration, and hemorrhage. The native bowel could not be salvaged so resection and jejunoileostomy were performed. Hematochezia and anemia resolved after surgical recovery.
DISCUSSION: This case demonstrates hematochezia, a relatively common pediatric complaint, which was suspected to be due to milk protein allergic proctocolitis and resulted in the missed diagnosis of a congenital enteric lesion. Unlike most cases of mesenteric duplication cysts, this patient had no palpable masses or abdominal distension. These lesions were detected by prenatal ultrasound but were dismissed postnatally. Severe microcytic anemia was the only sign of the severity of her illness and the need for prompt surgical management. Anatomic abnormalities discovered prenatally should be surveilled into infancy until they are resolved, corrected, or determined to be benign. Gastrointestinal duplication cyst(s) should be included in differential diagnoses for pediatric patients with unexplained hematochezia refractory to treatment.