| dc.description.abstract | BACKGROUND: The Centers for Medicare and Medicaid Services (CMS) introduced Comprehensive Primary Care Plus (CPC+) to improve the quality of primary care services nationwide. CPC+ utilization measures use a risk-adjustment model to predict utilization for different patient populations. Risk is determined using Hierarchical Condition Categories (HCCs), which are based on ICD-10 codes and patient demographics. Since patients with higher HCC scores are expected to have higher utilization rates, CMS uses these calculations to compare practices and categorize patients into “risk tiers,” which guide payments. OUSCM participates in CPC+ (Track 2). In order to track our patients’ emergency department utilization (EDU), search for patterns of use, and identify opportunities for quality improvement, we sought to determine (1) what associations exist between HCC risk tiers and patterns of EDU and (2) what patient characteristics are associated with HCC risk scores.
METHODS: We analyzed cross-sectional CPC+ data for fiscal year 2018 provided by CMS. We performed multiple linear regression, Tukey’s method, and independent-samples t-tests to explore possible relationships between EDU, HCC risk score and associated risk tiers (range 1-5), and patient characteristics, such as dual-eligibility status and age. The study population included 906 Medicare-only and 1173 dual-eligible patients aged 18 years and older attributed to the OUSCM Internal Medicine (n=1122) or Family Medicine (n=957) practice.
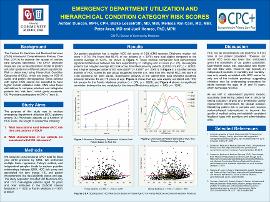
RESULTS: Our patient population had a median HCC risk score of 0.93 (CMS-reported Oklahoma median risk score = 0.74). We found that 56.4% of our patients were dual-eligible compared to the national average of 19.4%. Tukey multiple comparison test demonstrated significant differences between risk tiers and ED visits (p < .05). Dual-eligible patients had a higher average HCC risk score than Medicare-only patients (t(2072) = 8.491; p < .00001) and a higher average number of ED visits (t(2077) = 3.9577; p < .00001). Age was weakly correlated with HCC risk scores (r = .074, p = .0228). Density analysis of HCC scores by age revealed evidence of low-risk clustering for adults between 45 and 75 years of age.
CONCLUSION: HCC risk tier classifications are predictive of EDU rates in our patient population. However, our overall HCC score was lower than anticipated given the complexity of our patient population. Dual-eligible status was associated with higher risk and EDU rates. However, age–typically an independent predictor of morbidity and mortality–was only weakly correlated with HCC scores, suggesting clinicians may be undercoding encounters for adults between the ages of 45 and 75 years, which decreases revenue. | en_US |