Management of Endoleak After Abdominal Aortic Aneurysm Repair
| dc.contributor.author | Pham, William | |
| dc.contributor.author | Horst, Vernon | |
| dc.contributor.author | Pandit, Viraj | |
| dc.contributor.author | Kempe, Kelly | |
| dc.contributor.author | Nelson, Peter | |
| dc.contributor.author | Kim, Hyein | |
| dc.date.accessioned | 2020-07-07T14:59:52Z | |
| dc.date.available | 2020-07-07T14:59:52Z | |
| dc.date.issued | 2020-05 | |
| dc.identifier.uri | https://hdl.handle.net/11244/324956 | |
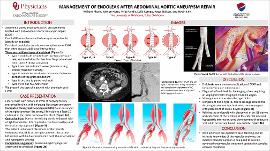
| dc.description.abstract | INTRODUCTION: Abdominal aortic aneurysm (AAA) represents a potentially life-threatening condition that requires proper surveillance and treatment. While AAA was historically treated by open surgical repair, technologic advances have resulted in Endovascular Aortic Aneurysm repair (EVAR) becoming the primary repair technique for AAA. Persistent endoleaks are a known complication of EVAR that often require additional intervention. We present a case highlighting the management of a Type 1B endoleak post-EVAR. CASE DESCRIPTION: Our patient is a 66-year-old male with history of EVAR at outside facility, and was evaluated in clinic with an enlarging iliac artery aneurysm. Computed tomography angiogram (CTA) demonstrated a 5cm aneurysmal degeneration of the right common iliac artery, most likely due to an endoleak in the distal portion of the stent (Type 1B). Due to the existing aortic endograft with a high flow divider, this required a combined axillary and femoral artery approach. The patient underwent placement of iliac branch endoprosthesis (IBE) at the right common iliac artery bifurcation with limb extension into both the external iliac and hypogastric arteries. Completion angiogram demonstrated successful extension of the endograft with exclusion of both the AAA and iliac aneurysm, preserved patency of the right hypogastric artery, and no endoleak. DISCUSSION: Endoleaks are a known complication of EVAR and frequently require intervention. There are multiple type of endoleak. Type 1 endoleaks denote leaks due to inadequate seal, and are divided further into 1A (proximal seal zone) and 1B (distal seal zone). Type II are due to branch vessel, type III endoleak are due to graft connection, and type IV due to graft porosity. The identification of location and type is frequently challenging and requires an angiogram. The management is based on the type of leak. Our patient had a type IB, due to leakage around the distal right common iliac limb. Relining the endograft with placement of an IBE device and extension of the stents into the external iliac and hypogastric arteries ensured development of adequate seal while preserving blood flow distally. With extensive pre-operative case planning and an intricate knowledge of the vascular anatomy, the modern vascular surgeon is equipped to provide advanced endovascular treatment options for complex vascular conditions. | en_US |
| dc.language | en_US | en_US |
| dc.rights | Attribution-NoDerivatives 4.0 International | * |
| dc.rights.uri | https://creativecommons.org/licenses/by-nd/4.0/ | * |
| dc.title | Management of Endoleak After Abdominal Aortic Aneurysm Repair | en_US |
| dc.type | Presentation | en_US |
| dc.description.peerreview | No | en_US |
| ou.group | Other | en_US |
Files in this item
This item appears in the following Collection(s)
-
Clinical Vignette Symposium 2020 [23]
The OU-TU School of Community Medicine's annual showcase of clinical vignettes from fellows, residents, and students.

Except where otherwise noted, this item's license is described as Attribution-NoDerivatives 4.0 International