| dc.contributor.author | Hilborn, Michael | |
| dc.contributor.author | Shapiro, Ekaterina | |
| dc.contributor.author | Hu, Tom | |
| dc.contributor.author | Wildes, Daniel | |
| dc.date.accessioned | 2020-05-05T19:37:42Z | |
| dc.date.available | 2020-05-05T19:37:42Z | |
| dc.date.issued | 2020-02-28 | |
| dc.identifier | ouhd_hilborn_reflexsyncopeinthe_2020 | |
| dc.identifier.citation | Hilborn, M., Shapiro, E., Hu, T., & Wildes, D. (2020, Feb. 28). Reflex syncope in the setting of deglutition: A case report. Poster presented at Research Day at Oklahoma State University Center for Health Sciences, Tulsa, OK. | |
| dc.identifier.uri | https://hdl.handle.net/11244/324200 | |
| dc.description.abstract | Background: Deglutition syncope was first identified by Thomas Spens in 1793 as a rare form of neurally-mediated transient loss of consciousness secondary to an atypical vasovagal reflex during swallow-induced esophageal dilation. Due to the lack of validated diagnosing criteria, detailed history is imperative to guide timely evaluation and management. | |
| dc.description.abstract | Case: A 58-year-old male with a past medical history of bipolar disorder, PTSD, anxiety, cocaine and methamphetamine use presented after a syncopal episode. He reported multiple syncopal episodes over the past five years associated with swallowing. During the most recent incident, the patient reported consuming food when he started feeling fullness in his throat, associated with lightheadedness and diaphoresis prior to a syncope episode. Patient's ED course was unremarkable with stable vitals without orthostasis, negative troponin, chest radiography and ECG. Patient was admitted for further syncope work up. | |
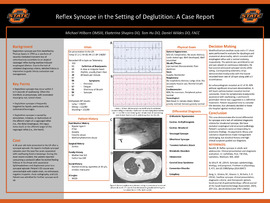
| dc.description.abstract | Decision-making: Modified barium swallow study and CT chest were performed to evaluate dysphagia and anatomical abnormality, which revealed mild esophageal reflux and normal anatomy respectively. The patient was allowed to eat. He was placed on continuous telemetry. Patient had several witnessed syncopal events while eating. Corresponding telemetry strips demonstrated bradycardia with a low of 10 bpm along with a 3 second pause. | |
| dc.description.abstract | Echocardiogram revealed EF of 35-40% with no significant structural abnormalities. Left heart catheterization revealed normal coronaries. Given his symptomatic bradycardia associated with swallowing, a permanent pacemaker device was suggested as the definitive treatment. Patient requested time to consider the decision, but ultimately decided to leave the hospital against medical advice. | |
| dc.description.abstract | Conclusion: This case demonstrates the broad differential for syncope and lack of validated diagnostic criteria for situational syncope. We have excluded esophageal and structural pathology. Patient's symptoms were corresponding to telemetry findings. His psychiatric illness and substance dependence made management challenging, but detailed history and high clinical suspicion guided our diagnosis. | |
| dc.format | application/pdf | |
| dc.language | en_US | |
| dc.publisher | Oklahoma State University Center for Health Services | |
| dc.rights | The author(s) retain the copyright of have the right to deposit the item giving the Oklahoma State University Library a limited, non-exclusive right to share this material in its institutional repository. Contact Digital Resources and Discovery Services at lib-dis@okstate.edu or 405-744-9161 for the permission policy on the use, reproduction or distribution of this material. | |
| dc.title | Reflex syncope in the setting of deglutition: A case report | |
| osu.filename | ouhd_hilborn_reflexsyncopeinthe_2020.pdf | |
| dc.type.genre | Presentation | |
| dc.type.material | Text | |
| dc.subject.keywords | cardiology | |
| dc.subject.keywords | bradycardia | |
| dc.subject.keywords | vasovagal | |
| dc.subject.keywords | deglutition | |
| dc.subject.keywords | syncope | |